
S3E4 Transcript - Roles of Professional Patient Partners in Engaging Children, Youth, and Families in Quality Improvement and Governance

Overview
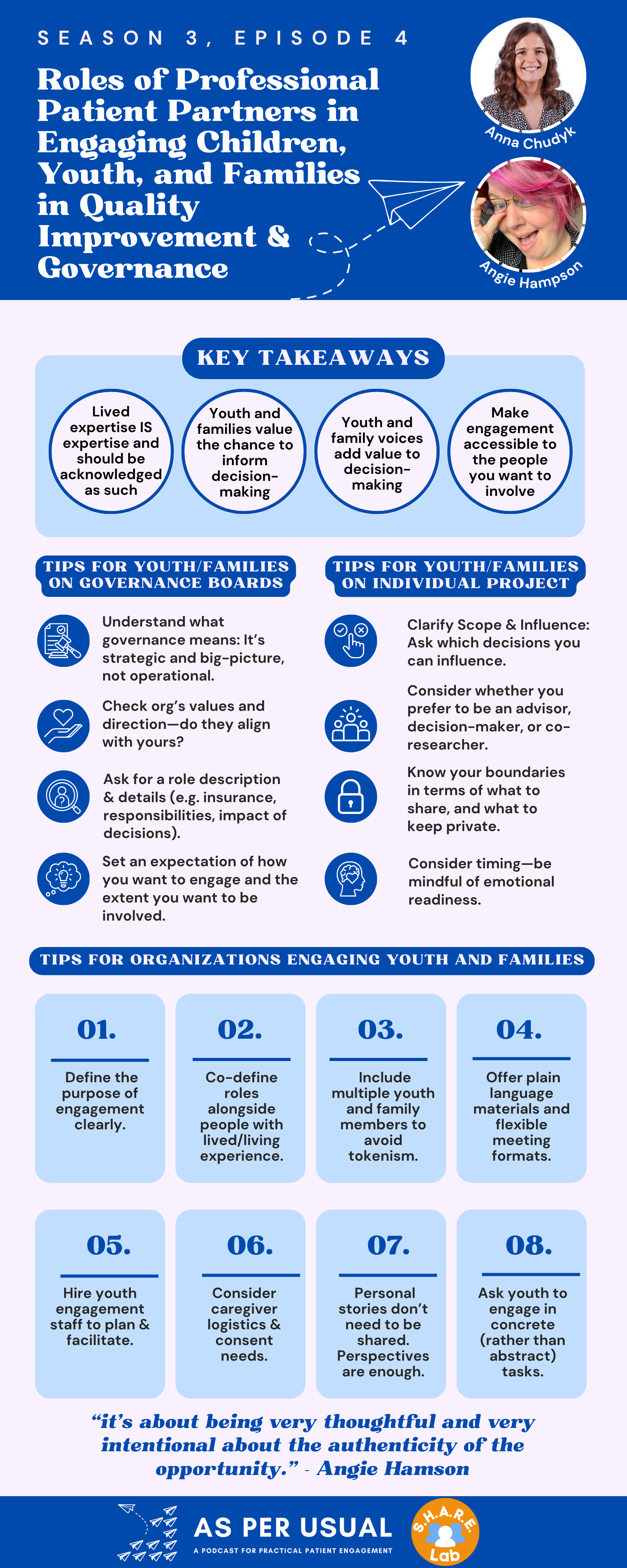
In this latest episode of asPERusual, host Anna Chudyk sits down with Angie Hamson, a powerhouse in the world of child, youth, and family engagement. Angie shares her remarkable journey from being the parent of a medically complex child to becoming a patient partner in volunteer and professional appointments - holding roles across advisory boards, nonprofit organizations, and health system staff teams. In sharing her journey, she also clearly details what it actually looks like to bring lived/living experience into professional roles—such as "patient partners in residence"—and why these roles matter.
Tune in to hear important insights on how organizations can move beyond tokenism to authentically integrate children, youth, and family voices across projects, governance, and strategic decision-making. You’ll also learn practical strategies for those hoping to enter the field themselves—whether as children, youth, or families with lived and living experience — and reflect on the importance of boundaries, support, and shared values. Other key discussion points include the role of privilege in shaping perspective, the importance of thoughtful engagement design, and how organizations can better engagement through compensation, recognition, and skill-building.
Whether you're a researcher, patient partner, the head of an organization, or just someone passionate about patient-centred care, this episode is packed with tangible lessons. So what are you waiting for? Keep reading below!
Meet our guests

Angie Hamson (she/her) is a Family Engagement Specialist at the Knowledge Institute on Child and Youth Mental Health and Addictions. She is the parent of a child with a complex medical history and is a patient herself. She has been a family advisor and patient partner for over a decade and has five years of experience as a professional engagement lead. Angie’s focus is on engaging people with lived and living experience in mental health and substance use health, people-centred care, and patient safety. She supports the Knowledge Institute’s Family Advisory Council and champions engagement with agencies across the province.
Contact the host: Anna M. Chudyk - anna.asperusual@gmail.com
Table of Contents
Coming soon
Resources
All of the resources below are free for everyone to read:
Transcript
Anna
Hi everyone, and welcome to season three, episode four of asPERusual, the podcast that explores practical ways to engage patients and the public in health research. I'm your host, Anna Chudyk. If you're new here, asPERusual is all about patient engagement in research, which means working with patients, caregivers and community members as partners in the research process, not just as study participants. These partners might sit on an advisory group, consult on a study design, or even join the research team itself. The important thing is, they help guide the decisions being made, and bring lived experience to the table in a real and meaningful way. We often refer to them as patient partners, or persons with lived experience.
Joining me today is Angie Hamson, a family engagement specialist at the Knowledge Institute on Child and Youth Mental Health and Addictions. Angie’s here to continue this season's focus on engaging children, youth and families in research. She'll be sharing her unique experiences as a patient partner, both in volunteer and professional roles, across the research and health care sectors. Thanks so much for being here, Angie.
To get us started, can you tell the listeners a little bit about yourself?
Angie
Absolutely. Thank you so much for having me, Anna. I really appreciate the opportunity to be on your podcast. My name is Angie and I am the parent of a child with a complex medical history. So my youngest son was born, I don't like to say birth defects, so I like to say that he came custom. He was born with a number of unique features and, spent quite a bit of time in the hospital in his first few years. Charlie had 12 surgeries before he was four, including open heart surgery multiple times and brain surgery a couple of times. He spent about six months in the hospital over the course of his first few years, one week here, two weeks there. His longest stay was 13 weeks in the hospital when he had a brain infection as a baby. So it's been an interesting experience for us, navigating the healthcare system with a child so young. And from my perspective, I really wanted to give back to the hospital, so I began volunteering as a family partner.
Anna
Thanks for sharing that, and I really love the way that you say that Charlie was born custom made. I think that's a very good way of putting it. I'm wondering, before we jump into engagement strategies, could we back things up a little bit? I know that in your engagement career, you've taken on many volunteer roles that eventually evolved into your current professional roles as well.
Can you walk us through how you first began applying your lived or living experience and volunteer roles over 13 years ago, and how that's evolved into professional paid roles over the last five years?
Angie
Absolutely. As I mentioned, with Charlie's complexities and time in the hospital, he had multiple life saving events. Another way to look at it is he had multiple life threatening events, but I prefer to focus on the life saving care that he received at the hospital. I was so thankful for the wonderful care that we received that I wanted to give it back, I wanted to pay back the hospital for everything that they had done for us, and to pay it forward to other families as well. I wanted to build on the many positive experiences that we've had, and I wanted to learn from some of the not so wonderful experiences, and some of the near misses.
So I started volunteering as a family advisor in 2011, and got involved with the family advisory council at my local hospital, our local pediatric hospital, CHEO, the Children's Hospital for Eastern Ontario. And that was a wonderful experience to be able to get involved with the advisory council to learn about the different processes and programs and initiatives and to be able to contribute to discussions at a meaningful level. I started partnering on a number of different projects throughout the Family Advisory Council and throughout CHEO, partnering on master planning and master programming and the Mychart User Advisory Group, which was looking at patient portals to electronic health records. I got involved in the perioperative patient safety team and a number of different ways to get involved throughout the organization. This was such a wonderful experience, I joined the Family Advisory Council executive and worked my way through, member at large to vice chair, and chair and then past chair, over the course of a 12 year span. I fell in love with engagement so much that I wanted to start giving back to other organizations as well.
So I began volunteering at a number of other organizations on some shorter term projects, like planning a conference, presentation, or getting involved with designing a course with healthcare can and things like that about patient engagement and patient experience and people centered care. So it was really a great opportunity to see what a number of different healthcare organizations were doing, both at the frontline level with CHEO and then again at the arm's length level with some of the other organizations that were supporting frontline organizations. I now sit on two boards of directors: (1) with PLEO, which used to be Parents Lifelines of Eastern Ontario, which is a peer support organization for families of children and youth with mental health and substance use, health issues and addictions, and (2) Patients for Patient Safety Canada, which is an organization made up of patients who have been harmed in the health care system, championing patient safety. So I've got a range of experience in the volunteer patient partner, family partner sector.
And then over the years, I started getting more and more involved. I went back to school when my son started kindergarten, got my degree, and really wanted to focus on health care improvement and how to contribute to organizations. So about five years ago, I was hired by Health Standards Organization to be an embedded family partner and patient partner on staff. So that that means I was hired not only to lead engagement as an engagement professional, but actually for that lens of lived and living experience within the health care system. Part of my role was to bring that lived experience, perspective, and voice onto the staff team, and contribute to our projects and initiatives. And part of my role was also to amplify the voices of others and support engagement with other family partners or patient partners, throughout the organization. And so that was my first foray into a professional patient partner or professional engagement lead position. I was there for about two years, two and a half years, transitioning to another position at Canada's Drug Agency, where I was more of an engagement lead, less for my lived experience lens. And I've now started with the Knowledge Institute on Child and Youth Mental Health and Addictions as, again, coming back to my roots as someone with lived and living experience to be on staff with that lens. So that's just a little bit of my history in a nutshell.
Anna
That's really fascinating, and if you don't mind, I'd really love to dig a bit more into your professional patient partner roles, since that's a perspective we don't often hear on this podcast. So I know that you touched a little bit on your roles and responsibilities within your first professional role, but,
I wonder if you could describe what your key responsibilities were in the other two professional roles that you had, and if you could maybe tell me a little bit about how you think your lived experience has shaped, or strengthened your work compared to someone in those roles without that experience?
Angie
Absolutely. So again, my role has been, sort of, to have the two hats at once. At one point, having that lived and living experience to contribute my own thoughts and my own perspectives on projects and initiatives, and to be embedded on the staff team, to be able to collaborate with colleagues on projects or initiatives or have those sidebar conversations before meetings or after meetings, just to bring up that need for people centered care and, and that need to highlight patient experience, family perspective, and things like that.
Anna
Would you say it was like being a patient partner in residence?
Angie
That's a great way of describing it. At Health Standards Organization, when I started, we had three part-time patient partners on staff, and it was great because we had different perspectives and different experiences, and mine was more as a caregiver, although I do have lived experience as a patient myself. The more extensive experience I have is as a caregiver. So to bring all three of those lenses to the work, to the team, we often collaborated on initiatives, and would have great debates about what we thought was important to highlight or some of the plain language and how to phrase things. It was wonderful to be able to work with a team, that really valued that patient perspective, and lived experience perspective.
I think it was a great way to work on projects that were maybe smaller as well, to still get that perspective of someone with lived and living experience, if it was just a quick update on something. Or a way to have that perspective from someone on the team who's more familiar with the projects and gets to know the ins and outs of of the work. But again, the other part of my role was to support engagement with people with lived and living experience or with family members, and caregivers in the work itself. And so there were times where I could be an ally or a champion for someone who was engaging in doing the work, and it was their voice that was being heard in the work. And so I think it's important to recognize that having someone on staff with lived and living experience is incredible. It's a wonderful asset to the organization, but at the same time, you still want to draw upon a wider pool of voices, because you don't want to tokenize the one person on staff as being the sole representative of patient and family perspective.
Anna
That's a really great way of putting it.
And did you hear from the other patient partners involved about whether they found any difference or whether it was more encouraging to actually have a person with lived/ living experience take on that liaison role, and for them to be able to work with you as opposed to somebody without that experience?
Angie
I think it enabled us to relate at a different level. When I would engage with people with lived and living experience in my second role with Canada's Drug Agency, I did a lot of 1 on 1 interviews with people. And so we'd talk in depth for an hour or two about their lived experience of a particular drug device or health technology and get a sense of how it benefited them, what the challenges were, and things like that.
And oftentimes before I would ask someone to open up, when we were first having our introductory calls, I would disclose a little bit about my experience as a patient and caregiver, and that often let people, first of all, it was I was trying to build more of a relationship with them and not be extractive and just swoop in, ask for the gory details, and then swoop off again. That's not what we want to do, we want to build a relationship of trust. We want to form a connection with somebody and and let them know that we are going to be asking some potentially sensitive questions. They don't have to answer anything they don't want to, and ensure their comfort and support throughout this process. And I think being able to disclose a little bit about my history at the beginning of a call set a bit of that tone of that expectation of reciprocity and the idea that I'm not expecting you to divulge your pain and your trauma and your experience, and not be willing to open up myself. And I think it sets the stage and, and I would speak with some people who would say, you know, you're a caregiver, you get it. And they would relate a little bit better to someone with that lived and living experience. And I would always say, you know, we have different experiences and I will never fully be able to understand what you're going through, or what you've been through, but hopefully I can relate a little bit. And I think we need to understand that everyone's experience is unique, and the best we can do is try to understand and relate as best we can.
Anna
And that flexibility and that ability to really relate and connect comes in handy, especially when you are doing semi-structured interviews where you can probe, you can change the script a little and really how “well” the interviews go actually does in large part depend on the relationship that's established between the interviewer and the interviewee, so that makes a lot of sense. I know on previous episodes I've mentioned that in a previous study, I co-led qualitative interviews with a patient partner (the late Mr. Roger Stoddard). At the end of the interviews, we asked all the patient partner participants how they felt about having someone representing the researcher lens and the patient partner lens jointly interviewing them. They had very similar things to say about how Roger and I brought different perspectives, and how the different kind of probing questions that we asked came at different angles, which resulted in a more holistic conversation.
Angie
Absolutely.
Anna
So what else do you think has helped you succeed in your professional patient partner positions?
Angie
I think having the support of my organization is a big factor. I think when you have an organization that really values a family perspective, caregiver perspective, patient perspective, that whole lived experience expertise, and recognizing that that experience does give you expertise in this area, that is incredibly valuable. I think being able to have positions where you have people that are part-time, for example, might help some people who are managing their own health conditions or caregiving responsibilities, to transition into that part time role with support, and still manage their day to day commitments. Whether that's health care appointments for themselves or their loved ones or caregiving tasks.
So that's another consideration for organizations looking to bring on people with lived and living experience is to look at, or to consider — the needs of the individuals as well as the needs of the organization. Because I think to partner with anyone with lived and living experience, it needs to be able to work for the individual, as well as the organization. I think having a supportive team and having people that will go to bat for you is really important as well. So having managers or supervisors or directors who understand the needs of the individuals with lived and living experience, but also champions their expertise throughout the organization is really helpful and one of the stepping stones to success, I think, in incorporating one of these positions into your organization.
I think having the support of my family is incredibly important as a caregiver. I do draw upon my lived and living experience with my son. And my son Charlie is now 15, and we've talked about what he's comfortable with me sharing about his past and what he'd prefer me to not discuss. And so there are things that I have boundaries around or limits around about what I'm comfortable sharing. And in Charlie's mind, as he put it. What did he say? He said, I don't remember the early days, so that was your trauma, not mine. I think that he's oversimplifying things a little bit in that he certainly did experience trauma, as a youngster with a lot of adverse events in early childhood, but he doesn't remember a lot of them consciously. And so he's quite confident with me or comfortable with me sharing some of those early experiences that he doesn't remember, but I generally don't talk about his current situation as much, because that's more sensitive to him. And so that's more about his actual reality today as opposed to his history. So having family members who support my role and support me in sharing this information is important too, because I would never want to share anything without my son's consent.
Anna
That makes a lot of sense, and Charlie sounds like a very wise young man. Something that I love about this podcast is that every conversation pushes me to think about something that I haven't thought of before, in terms of engagement, which is saying a lot, because I spend a lot of my free time thinking about engagement and talking about it whenever I can. I just love all things engagement. But, something that I haven't thought about in terms of the professional patient partner role is really the power of having that patient partner in residence and knowing that your organization, if they do need something quickly vetted, or want to check some initial ideas, they have someone that they can turn to that can really represent the patient partner perspective, in a way. But that's also very daunting, because for a project you're chosen because of specific lived/ living experiences, whereas for an entire organization, it just seems like they could be looking for a lot of different perspectives.
What do you think about you personally has made you a really strong fit for that role? I'd assume some of it is all the many years you spent in volunteer roles, but what is it?
Angie
I think from my perspective, there's benefit in looking at the breadth of my experience over the years with my son. One of the reasons I volunteered at CHEO for 12 years was that we had continuing experience throughout the hospital up to and including today. Charlie will continue to be seen by the health care system, into adulthood, through the pediatric system and then transitioning into adult care, where he will have ongoing follow up for certain chronic issues. And so I think having that diversity of experience, where he was seen in 12 to 15 different clinics as an infant and toddler. So to be able to have some of that breadth of experience for my volunteer role at CHEO, was very helpful to me to be able to bring in perspective from a lot of different areas of the organization.
And I think when you're looking to transition into that professional role, having that breadth of experience in a number of different areas was really helpful to me. I wouldn't say that I have experience in all areas because of course I don't, I'm one person. I don't represent all patients, all caregivers. I speak for myself and my own experience, and that is the lens that I bring. But I do try to think a little bit more broadly, when I'm looking at projects or initiatives. When I'm asked a question about access, for example, I might say, well, I have benefits. So the cost is minimal to me for this prescription. But for someone without benefits, this would be a barrier, right? And so it's a bit more broad than my own experience. Or I live in a semi-rural area, developed outside the city where I don't have public transportation. So from my perspective, I can get to the city to get to the organization, to get to the hospital, but that's because I have a car, and I have the privilege to have a car and to be able to afford insurance and gas and all of that stuff. But someone in a rural, remote community may have an eight hour commute or a flight to get to the hospital, the same one that takes me half an hour. So I think being able to draw upon your own lived and living experience and recognize that you don't represent the the entirety of your population. But at the same point, try to think a little bit more broadly than than your own privileges and recognize and say, well, I have this experience, but others may have a different experience and that might be a barrier to that.
Anna
I really love the way that you put that. And I think a strength that I was born with is that I've always been able to try to put myself in other people's shoes. What's really elevated that skill/gift — and has also helped me to share it with others and encourage them to better consider other people's perspectives as well — is to reflect on my own personal privilege. So, to go through and to really think about what circumstances allow me to live the life that I have, to express gratitude for them, and then recognize what it could be like for others who don't share these same privileges. And that right there is a very powerful way to tap into the potential perspectives of others. Obviously that doesn't replace speaking to these people and having them bring their perspective directly. But it's a good way just to get that conversation and those thoughts going.
Angie
Absolutely. I think it's so important to think, beyond yourself, and to recognize those privileges that we have.
Anna
Yeah, it's not just something that the millennials say in terms of checking your privilege, there's a lot of power and thought behind it. I have one last question before we shift into engagement strategies. And I know that you've covered a lot of this already, but I think it could be nice to reiterate your answer, succinctly or in one place, in case somebody is listening and is starting to think about advocating for a professional patient partner role in their organization, or perhaps they want to advocate for themself for such a role.
Why do you think it's important for institutions, organizations, or research teams to hire people with lived/ living experience into professional roles like engagement specialists, leads, coordinators, patient partners in residence, etc..?
Angie
I think it's important for organizations to understand the value that lived experience brings, and that it's an expertise that people develop over time in the same way that someone might study a condition or an illness. We live it, right? And we experience not only the condition or the circumstances, but the system navigation and the access, and the barriers, and the challenges, and the successes. And we build those relationships with clinicians and with coordinators. And we understand the system in a different way than a healthcare professional or an academic might.
I think to bring together researchers, frontline staff, management, leadership and people with lived and living experience, brings together a whole bunch of different perspectives that can create something absolutely beautiful. When you bring all of those perspectives together, I think you get a far more nuanced understanding of an issue. And so bringing someone onto your staff team that has lived and living experience, builds a closer relationship with that individual.
For example, one of the things that I did when I was working at Health Standards Organization was facilitate a community of learning. So like a community of practice, but a community of learning where we would come together with staff (I think on a bi-monthly basis), and have a conversation about various issues that were affecting healthcare at the time or the patient experience/people centered care. And so we had a wide range of conversations over time, which contributed building these relationships with staff and all of us coming together. This was over Covid, so it was all virtual. We were able to discuss caregiving policies, we were able to discuss access and barriers, and wait times and things like that, that were affecting people on the ground today.
It was wonderful to be able to facilitate some of these discussions and the sharing and the opening up that people would do in these sessions, highlighting their own experience with their loved ones, as caregivers themselves or as family members of people going through long term care during Covid. To be able to have some of these discussions, we would talk about different topics at different times. Some of it was more focused on people centered care and patient experience, some of them were more focused on engagement. But, as a staff member, one of my responsibilities was to build those relationships within our team and to give people exposure to some of these ideas and strengthen their capacity to engage with our family advisors or patient partners in their project work.
Anna
That makes a lot of sense. And so you could help them both brainstorm how to do so, also navigate probably common concerns that they came across, and help them get more use to the types of considerations that they should bring to their engagement as well, right? So it's that whole familiarizing yourself with how to think and how to approach things that can only come from working with others with different experiences to yours, and that have experiences more closely aligned with the ones that you are trying to connect with.
Angie
Well, and we would come up with strategies on how to engage. We would provide training, or orientation and onboarding to committee members, for example, coming from the public to participate on our committees. We would provide information about people centered care and patient engagement to everyone, so that everyone was starting on the same level playing field about the value and benefits of patient engagement. That way, people weren't walking into an environment where people were unfamiliar with engagement. We wanted to make sure that people had the same baseline.
Anna
We've heard a lot throughout the seasons about the importance of proper onboarding, whatever the engagement setting is as well.
Angie
Absolutely.
Anna
So now to shift gears a little bit and start focusing in on engagement strategies. Let's reground ourselves in the experience that you bring
Let's reground ourselves in the experience that you bring
Angie
My early engagement work was related to general health care experience. It was about navigating through the health care system, within the pediatric health care context. A lot of our experience in the early days was more physical. Although there was a mental health component as well, the more complex issues were more physical, and so that's how I began my engagement experience. Then, I ended up working with a number of different organizations on more general issues — for example, virtual health or patient safety — which were all related to a particular project with a particular focus.
As I transitioned into my professional role… well, my role at Health Standards Organization was on standards development or supporting engagement and standards development. So we were looking for people to engage with us that had a range of different specialties or experience in specific areas. For example, if we were working on a health care standard for long term care, then we were looking for people that were family members or residents themselves of long term care. So that was that specific lens for that particular project. And I think it's important to recognize the need for that specific experience and expertise, as you say, when you're working on a specific project to have that particular lens. While we all may have different levels of health care experience ourselves, when you're working on a project focusing on a specific topic, you're hoping to connect with people with experience of that specific area.
My latest role, now with the Knowledge Institute, is focused on mental health. And part of the reason I was so excited to take this position was because I was able to marry my lived experience of pediatric mental health with my professional experience as an engagement lead. So that is my area of focus now, but I've had a a more diverse background over the years.
I think quality improvement is another area that you mentioned, that I think is really important, and that I think patient/family engagement is an incredible piece of that. Because, again, you want to be able to consider all the different perspectives of your service. And if you're evaluating how your service is delivered, I think you're falling short. I think you need to look at how your service is received, and I think that's a big difference. So what we think about in our policies and procedures and processes, is that we expect to be able to deliver a service a certain way. But, we need to understand what is needed by the population and how the services are received, where the gaps are, and things like that, when we're looking at quality improvement. I was actually very fortunate to be participating in some quality improvement initiatives in my volunteer days at CHEO, and they were running a Lean Six Sigma training course for their staff, and invited me along so I was able to actually get some Lean Six Sigma training as a volunteer patient partner.
Anna
Could you explain what that is for people who are listening and unfamiliar?
Angie
Absolutely. It's a quality improvement initiative and training — it's a methodology about how to improve systems and processes. It's about minimizing waste and ensuring consistency of processes throughout an organization or a system. And so it's really interesting. It's based on, I think, the manufacturing process back in the days, early in the automotive industry, I believe. And so I sometimes struggle with how some of those philosophies translate to healthcare because as a patient or family member, you know, we're not inanimate widgets moving through a process. We are active people with agency, and preferences and priorities and needs. So we need a system that is responsive to those needs. But I think it's really important to look at quality improvement through that people centered lens and to recognize the importance of that family or patient perspective in those processes. We do need to standardize processes for safety and quality, but its important not to lose that customization or that personalization, from that family or person centered lens.
Anna
I love it. And another big takeaway that I got from your answer to my question is that truly one of your superpowers is the breadth of experiences that you have obtained from navigating the health care system through so many different services with your son. As well as, on top of that, all the different perspectives that you've been privy to as a result of your numerous volunteer roles and your professional roles as well. So then I think the natural next step for us is to talk strategy.
What tips do you have for health care or research organizations that are looking to engage children, youth, and families in their governance structures?
So I know you've said that you worked with individual projects, but you've also worked at the level of actually the Executive Council and the governing of the organization. So let's start there before we move into individual projects.
Angie
Absolutely. I think it's really important to understand the goal of engagement when you go about planning on how to engage. I think we need to be very intentional about what we're hoping to accomplish with engagement, as an organization. And so, you don't want to invite somebody onto a board to be a token patient, or a token family member, just so that you can check the box and say, well, we've got a patient on the board, so everything's fine. I think you need to look at what the purpose is, what their role is going to be, and you need to co-develop this with people with lived and living experience. So your board needs to potentially talk to people with lived and living experience to see how they see a board role progressing or rolling out.
I think it's really good to look at having 2 or 3 people with lived or living experience, on a board or advisory role, as opposed to having only one. Because again, then you end up being sort of pigeonholed into, well, you're the family member, what do you think? As opposed to having a robust discussion with multiple people with lived or living experience who can contribute different perspectives on issues. So I think it's really important to understand the purpose, to understand the role that someone's going to fill, to co-develop that together with people with lived and living experience, to understand that experience that they bring does give expertise that you will never find on a resume, right? There is so much that we can learn from people with that lived and living experience, that is not secondary to professional credentials. It is hard earned experience and expertise.
I think the other thing to consider is how to support people with lived and living experience to participate in a governance structure. Ensuring that there's plain language documentation, for example, accommodation for timing, and methodology of the meetings. If you've got somebody coming in from a further distance from your organization, can they zoom in or participate virtually? What kind of supports can you put in place if somebody is experiencing distress at the conversation, and things like that. So I think it's about being very thoughtful and very intentional about the authenticity of the opportunity.
Anna
I love how you break your answers down into easy to follow categories. As I've probably said before, I thinkin pictures, so your words immediately go into little thought bubbles as you speak. People always ask me this question and it sometimes stumps me, so no worries.
But can you think of an example of when you've seen patient engagement in an organization’s governance go really well, or really have an impact on some sort of an output of the organization, or maybe its very structure?
Angie
Well, I sit on the board of an organization that does peer support for families of children and youth experiencing mental health, or substance use health, or addictions issues. I know that we were really involved in coordinating a fundraiser. Now, I joined the board in September and the fundraiser was October, so I didn't have a lot of time to get particularly involved other than attending the fundraiser and promoting it on social media and sending it to my friends and family and things like that. But I think it was really great to get the perspectives of people with lived and living experience in the coordination of the event. We had speakers sharing their lived and living experience of the service. We had peer supporters who shared their experience. We had an MC whose daughter performed some music, original songs that she had written about her mental health. And it was just a wonderful experience to see everybody coming together to make this event meaningful to people, as opposed to simply coordinating a fundraiser that was corporate and very cold. This was a very warm and welcoming environment that had that lived experience perspective. It also had wonderful food, and art, and an auction. But to see everybody highlighting their lived and living experience and being vulnerable was particularly powerful.
Anna
Love it, and I love how you described that people with lived/ living experience help make the event be meaningful, and not just necessarily full of bright lights and shiny things.
Angie
Exactly.
Anna
So digging in a little bit further, moving away from the governance structures,
What does meaningful engagement of children, youth and families look like at the level of individual initiatives/projects?
Angie
I think there's some very similar overlap in some ways about documentation and timing of meetings and things like that, to make things convenient or accessible to people. But I think you also need to understand, and maybe this applies to the board as well, power differentials, and the ownership of the project, and who is responsible for making decisions. On a board, everyone should have an equal vote, but on a project team, there may not be the same feeling of impact for a family member if they don't see their contributions influencing the outcomes of the project. That can be very frustrating or disempowering for people. So recognizing what is within scope of the project and what people can actually influence, I think is really important.
All projects have constraints, right? All projects have a budget. And there's certain things that are mandated, and there are certain things that are legislated, and we can do this and we can't do that. So understanding where the sphere of influence is on a project and being able to direct people's energy effectively to something that can actually influence is really important. I think respecting people's backgrounds and expertise and the experience that they bring is really important. So understanding that when people are sharing their perspectives, they may not want to share their story or divulge their history. They may want to come and be able to share their perspectives on things, drawing on their lived experience, but not necessarily having to open up, to be someone's inspiration or be forced to be vulnerable in that moment. They may want to come and work on the project, share their perspective, and not necessarily have to go into the experience themselves. I think we want to recognize that people are more than just their stories.
Anna
Really well put. And I wonder if within that, going in a little further… well one of my anxieties with moving into engaging children, youth and families is the actual engagement of younger populations, because it's something that, as I've mentioned before, I have not previously done. I have one scarring experience that I need to let go of, of being a lunchtime monitor for youth, that did not go great.
So do you have any specific strategies, or things that you've seen, that work when you're trying to engage these younger populations in a quality improvement initiative or a research study or something?
Angie
I think there's different strategies that work at times and others that don't work at times. And sometimes it's hard to know which strategies to employ at which times. I think one of the things that where I work now, The Knowledge Institute, does really well is we have youth advisors on staff as well. Currently we have two youth advisors on staff that have lived and living experience, who are in their early 20s and are wonderful people who have great experience in facilitating groups and connecting with young people to be closer in age and to be able to relate a little bit better.
Again, I think it's tricky to work with young people. It's one thing to work with university students, another thing to work with adolescents, and yet another thing to work with children. So I think it’s important to look at how to connect with people in different ways, different times, and at having different people potentially involved in some of these engagement efforts. I know my son Charlie now is involved in CHEO’s Youth forum. And so he's engaging on an advisory committee, primarily made up of adolescents 12 to 18. Some of the things that have worked well with him, for example, are the ability to participate virtually because I don't have to take time off work to drive him to an in-person meeting. At the same time, I think when they do have an in-person meeting, it enables some greater connections to be made. So having a balance of those two modalities can be helpful.
He's gone for tours of a certain area, when they were looking at signage in their perioperative area. And so the youth all went for a tour, and Charlie's had 24 surgeries now, so he has been in that surgical area many times. But they were able to look at concrete things as opposed to abstract. They were able to walk around the space and say, now what do you think? Is this signage clear? Does this tell you where you're supposed to go? How do you feel when you're in this room? As opposed to looking at what's the new mission, vision and values, right? So sometimes having something more concrete can be easier to respond to.
When Charlie was little, when he was six, seven, eight, I remember CHEO was looking at their new whiteboards for the patient rooms, and they sent around six pictures of different whiteboards and had us vote on our favorite. And so I pulled it up on my phone, and I showed Charlie the six whiteboards at six, seven, eight years old. And he picked his favorite, so that's who I voted for, he had my vote. It was something more concrete and more tangible at a very young age, he was still able to share his thoughts. When asked, how do you feel when you come to the hospital? And how do you feel when you talk to your doctors or your nurses? That was harder for him to express himself in those: I feel fine, I feel fine. Right? It's okay. It's all good. But to be able to have something more concrete, that was easier for him to visualize. That was one strategy that I know worked for him. I think it's definitely tricky to build relationships with an audience when there is such a great differential and especially a power differential between a researcher or manager or staff or a clinician and a family member, but especially for a youth or a child.
Anna
Thank you, that's really helpful. And my three key takeaways that I got from what you said are:
We always talk about the importance of engagement liaisons within, what I primarily work with which is the research setting (although I do do stuff with health services as well). Based on what you said, it’s important to push yourself to perhaps hire someone who is a younger engagement liaison that has familiarity, and maybe previous experience actually engaging as a child as well, to help plan and lead those sessions.
It’s important that children/youth are able to ground in more concrete questions/things… things that are tangible that they can more readily reflect on and provide their perspectives on.
Always consider the caregiver as well, and what impact or requirements the child's engagement poses on the caregiver who will have to be taking them to the different engagement opportunities.
Thank you. That's really helpful. Flipping the script a little, now that we've talked about what tips you would give organizations for engaging children, youth and families,
What advice would you give to children, youth, or families who are interested in getting involved in the governance of health care or research organizations?
Angie
Again, if we're looking more at the governance level, at the boards and leadership of organizations, I think it's really important that families, children and youth are aware of what governance means, and the type of work that they would be doing on a board. It’s important that they realize that here, they're not necessarily going to be engaging in projects or initiatives or service delivery or wait times or intake processes. They're going to be looking more at strategic directions, and budgeting, and any major concerns or reputational risks to the organization. And so I think it's important for people to understand the type of work that they're interested in and where their skills are.
For example, I really love advisory work, and I want to stay involved in advisory work. I don't just want to work at a board level. I like contributing to strategic directions, building that strategic plan, looking at how the organization might be operating in the next five years, and looking at how we're going to work together as an organization. But, these aren’t conversations about what the waiting room looks like at the hospital emergency department, right? Or what services can be delivered to support people waiting for 18 hours overnight when there's no food. You're not talking about something that's front line for people. And so I think setting those expectations of how you want to engage, and at what level, is really important when you're looking at how to engage with an organization. You want to make sure that your understanding of the role is appropriate.
You also want to look at the mission, vision, values of the organization and their priorities. Do they align with your own? Is it an organization that you have had services from, or is it an advocacy organization for a condition that is something that is familiar to you, or a research organization that’s researching issues or health care conditions or treatments that are relevant to you? I think it's really important to understand where an organization is going, to see if that is something that is important to you and aligned with your priorities.
I think you need to ask for a clear description of the role. From a board perspective, again, making sure of things like your responsibility and personal liability if something happens within the organization. Is there liability insurance for board directors, for example, that's a practical thing. But that was one of my questions when I was joining a board — what happens if something happens and the organization is found to be responsible for something horrible? What is my responsibility as a board director? And so wanting to ensure that I was protected as well.
Anna
These are really important considerations, and some of which I haven't thought of at all. Building off your previous answer, I also think it's probably important to determine what actual impact or power you hold as a board member as well, right? So are you there just as a token person, or can you actually have an impact on the direction, which may be harder to get from the organization? But you could perhaps figure some of this out when you look at the roles, or perhaps by speaking to other members as well, just to get their take.
Angie
Absolutely. And I think as a board member, recognizing that you are one of the decision makers at that point, at that level, and that you have an equal vote to other people. However, at the same time, you're one vote of the board. And so while you can contribute to decision making, the responsibility isn't on you to approve the budget on your own, for example. You're contributing to decision making, but recognizing the limitations on your influence as well.
Anna
So then again, moving down from the governance level:
What tips would you offer to support families or youth that are interested in engaging in more individual level research studies or quality improvement initiatives?
Angie
Again, there's some overlap with aligning your priorities and setting clear expectations or asking for clear expectations of roles, responsibilities and support. But again, understanding the project, understanding the scope and understanding the deliverables:
What is in your ability to influence?
What is the product that you're going to be to be developing or releasing at the end? Is it a new program? Is it a report? Is it binding? Is it not?
Is there decision making or are you contributing to something?
What level of engagement is it for you? Are you advising a decision maker or are you one of the decision makers approving a project, or things like that? Are you contributing as a co-author to a paper, or are you involved in designing a new pathway care pathway?
How do you get involved in determining the research question versus just reading over the documents to ensure plain language?
There's a number of different considerations for how you're going to get involved, what you're going to be able to influence, and what your role is going to be. I think the other thing to think about that's really important for children, youth and families is, like I touched on earlier in my conversation, is your personal boundaries. Recognizing, first of all:
When is the event happening?
Are you are you involved in something, and it's a really sensitive time for you because it's coming up to an anniversary of a trauma?
Or is it is it coming up to another surgery or intervention that might be more sensitive to you?
Is it something that you're comfortable sharing about? What are you comfortable sharing? What's off the table for you?
What level of information are you prepared to share? And what is something that you want to keep private?
What do you have consent to share as a family member? What do you need to keep close to yourself?
So I think it's understanding the scope, what you can influence and what you're comfortable sharing are to me the key big ones
Anna
I love it. And so as we wrap, I'm going to ask you two more questions. The first one being one that seems to stump a lot of guests, or they always say, well, I don't know, there's so much. I ask the question though because I like to give the power, in a way, of the story back to the person that came on, and to really give them the opportunity to ensure that their key messages came across clearly.
So are there any key takeaways that you hope listeners leave with, after listening to your episode?
Angie
You know, we haven't really touched on this, but I think the idea of just engaging early, engaging often, and engaging in multiple ways across the lifespan of your project. If you are coordinating, if you are leading an organization and you're looking at developing an engagement strategy for your whole organization, I would say look at how to engage in different ways and in a fit for purpose way across your organization at the project level, at the community level, at the governance level. Look at how to involve people at all sorts of different levels of the organization. And, to co-develop those strategies with people with lived and living experience, so you're not telling them how to engage, you're asking them how to engage.
Anna
Love it.
Is there anything else that we haven't touched on yet that you'd like to share before we close?
Angie
I think you've done a great job of giving an overview. I think one aspect that we haven't covered is compensation, but I'm sure you've talked about that many times in other episodes. So I think one of the things that's great for reducing barriers to engagement and increasing respect is that acknowledgement piece — whether it's:
honorariums and reimbursements
recognition as co-authorship or being listed on people's websites as family partners or patient partners
sharing opportunities (like I said, when I saw doing quality improvement as a volunteer patient partner, I had the opportunity to take part in a professional development opportunity that the staff were taking)
identifying other ways of recognizing people that are partnering with you, to really show them appreciation in the way that matters to them, whether that's a reference letter or a public LinkedIn acknowledgement or a private thank you letter. Something to demonstrate your appreciation for their time, effort and expertise.
Anna
I think a part of that as well is having that initial conversation with the patient partner and asking them, what are you hoping to get out of this? Because as we learned in previous episodes, patient partners often join because they want to give back and make a difference. When it comes to youth (and other populations as well), they also typically want to build certain skills or get experience in certain areas, that they can then use to move into another position or as a stepping stone towards somewhere/something else. So in addition to compensation and reimbursement, I think it's also important to figure out that skills piece as well, so that you can help ensure that people are able to get those skills if possible.
Angie
Absolutely. I know my son really appreciates his volunteer hours from the youth forum, because that's contributing to his high school requirements. What’s important is that it's valuable to the individual.
Anna
Exactly. That's such a big part of engagement, isn't it? Focusing on that individual and what's important and valuable to them. What they want to bring to the experience AND get out of it.
Angie
Absolutely.
Anna
Well, thank you Angie, so much, for coming on to the podcast today. I really loved this conversation and I definitely learned a lot from it. And thank you, listeners, for tuning in. As we wrap, I'd like to take a moment to acknowledge Briana Kelly and the George and Faye Center for Health Care Innovation for their help with editing this season’s episodes.
Next time you're on your phone or at your computer, please do check out our website, asperusual.substack.com for resources from today's episode, as well as interactive transcripts from this and previous episodes. While you're there, please be sure to subscribe to our podcast newsletter, as well as to subscribe to the podcast in general through wherever it is that you download your podcast episodes from. This helps other people find the podcast as they're scrolling through. If you'd like to contact me, please shoot me an email at Anna.asperusual@gmail.com. And do be sure to add me to LinkedIn by searching Anna Chudyk — C-h-u-d-y-k. Thanks so much for tuning in! And until next time, let's keep working together to make patient engagement and research the standard or asPERusual.
Loved this podcast Anna, Helpful “how to” engage as a professional, as a Mom and as a care partner/patient. Sensible, down to earth, thoughtful strategies. Thanks